

Even as the United States mounts more than half a million deaths from COVID-19, states continue to pass laws restricting access to reproductive health care, according to newly updated data released by the Center for Public Health Law Research Policy Surveillance Program on LawAtlas.org.
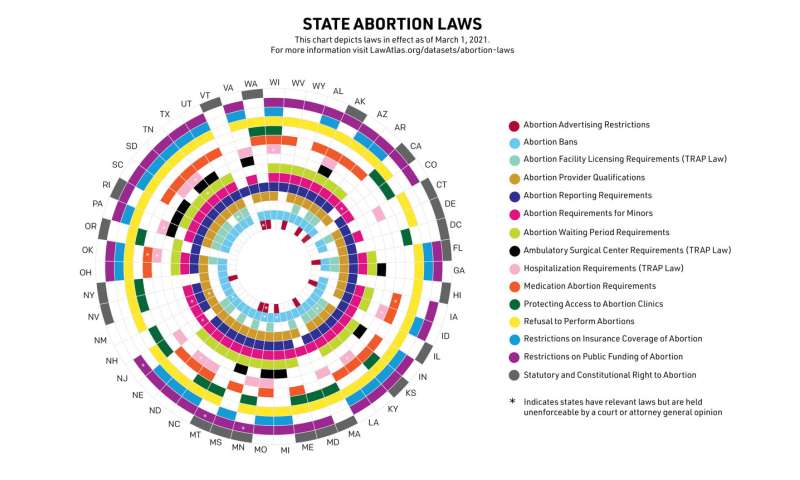
Analysis of the data, which capture state statutes, regulations, and court rulings in 15 different legal areas related to abortion across 16 datasets, from December 1, 2018, through March 1, 2021, finds changes in the legal landscape restricting access to abortion services. It also shows legal barriers to medication abortion and telemedicine that could otherwise be used to safely expand access during the pandemic and in general.
“We are now in our fourth update of these datasets since 2018, and we’re consistently seeing state legislatures chip away at access to essential abortion services,” said Adrienne Ghorashi, JD, program manager at the Center and lead researcher on the Abortion Law Project. “Instead of working to ease the burdens of the COVID-19 pandemic, some states have chosen to continue adding legal, financial, and logistical hurdles to abortion care, particularly for those communities most impacted by this public health crisis.”
As of the latest update on March 1, 2021, the researchers report:
- Medication Abortion Reversal Laws. Ten states now have “medication abortion reversal” laws that require providers to inform patients it may be possible to reverse a medication abortion, regardless of the fact that there is no medical consensus on whether that is possible or safe. These laws have been enjoined in three states: North Dakota, Oklahoma, and Tennessee.
- Access to Medication Abortion. On January 12, 2021, the US Supreme Court reinstated the FDA in-person requirement for mifepristone, again requiring patients to visit a clinic to obtain medication abortion. There are currently seven states where telemedicine for medication abortion is explicitly prohibited, thirteen states where the provider must administer medication abortion in-person, and ten states where a provider must conduct an in-person exam before administering the medication. These laws may still apply even if the federal government lifts the mifepristone Risk Evaluation and Mitigation Strategy (REMS) requirement.
- Fetal Heartbeat Bans. Nine states have fetal heartbeat bans, which ban abortion before many people even know they are pregnant, but all of these bans are currently unenforceable. South Carolina passed a fetal heartbeat ban just last month, which was also immediately blocked by a US District Court.
- Reason-Based Bans. Fifteen states now have laws banning abortion based on specific reasons, such as race, sex, fetal anomaly or disability, or a Down syndrome diagnosis. One-third of those bans have been enjoined by the courts.
Massachusetts recently expanded access to abortion services. The state’s ROE Act, passed in December 2020, guarantees a statutory right to abortion, removes parental consent requirements for 16 and 17 year olds, removes a law that permitted only physicians to provide abortion services, removed a 24-hour waiting period, and added an exception that would allow termination in the case of fetal anomaly after 24 weeks of pregnancy.
“In an ongoing pandemic, it would be our hope that more state and local governments act to increase access to critical health care for their residents, as Massachusetts recently did,” said Ghorashi.
The Abortion Law Project is maintained by the Policy Surveillance Program of the Center for Public Health Law Research in collaboration with subject matter experts from Resources for Abortion Delivery (RAD), Guttmacher Institute, American Civil Liberties Union (ACLU), Center for Reproductive Rights (CRR), National Abortion Federation (NAF), and Planned Parenthood Federation of America (PPFA).
Source: Read Full Article