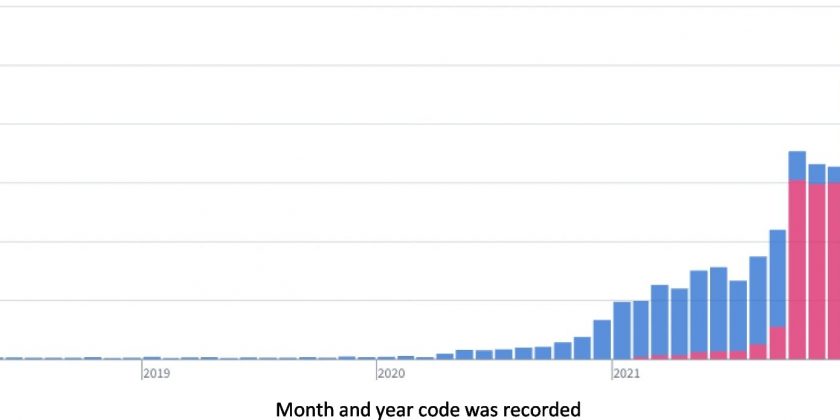
 as a placeholder code to signify long COVID. As this code is not specific to sequelae of COVID-19, this figure shows consistent but infrequent use during two pre-pandemic years. Use of B94.8 ramps up in Spring of 2020, suggesting increased recognition of long COVID by providers. However, upon its release in October 2021, U09.9 supplants B94.8 in terms of usage frequency. Credit: BMC Medicine (2023). DOI: 10.1186/s12916-023-02737-6")
Black and Hispanic Americans appear to experience more symptoms and health problems related to long COVID, a lay term that captures an array of symptoms and health problems, than white people, but are not as likely to be diagnosed with the condition, according to new research. The findings—from two different studies by NIH’s Researching COVID to Enhance Recovery (RECOVER) Initiative—add to a growing body of research aimed to better understand the complex symptoms and other issues associated with long COVID that millions have experienced.
“This new evidence suggests that there may be important differences in how long COVID manifests in different racial and ethnic groups,” said Mitchell S.V. Elkind, M.D., a professor of neurology and epidemiology at Columbia University, New York City, and chief clinical science officer for the American Heart Association. “However, further research is needed to better understand the mechanisms for these differences in symptoms and access to care, and also if diagnostic codes assigned by clinicians may play a role.”
In one analysis, published in the Journal of General Internal Medicine, researchers looked at the health records of 62,339 adults who received a positive COVID-19 test at one of five academic health centers in New York City, all between March 2020 and October 2021. They tracked the patients’ health for one to six months after the positive test and compared the findings to 247,881 adults who never had COVID.
Among 13,106 adults who had severe COVID that required hospital care, the researchers found Black and Hispanic adults were disproportionately represented. Of those who had these severe cases, for example, 1 in 4 were Black adults, 1 in 4 were Hispanic adults, and 1 in 7 were white adults.
In the months following infection, Black adults with severe disease were more likely than white adults to be diagnosed with diabetes and experience headaches, chest pain and joint pain, but less likely to have sleep disorders, cognitive problems, or fatigue. Similarly, Hispanic adults who required hospital care were more likely than white adults to have headaches, shortness of breath, joint paint, and chest pain, but less likely to have sleep disorders, cognitive problems, or fatigue.
Similar patterns emerged among people with mild to moderate disease. Among patients who were not hospitalized, Black adults were more likely to have blood clots in their lungs, chest pain, joint pain, anemia, or be malnourished. Hispanic adults were more likely than white adults to have dementia, headaches, anemia, chest pain, and diabetes. Conversely, white adults were most likely to have conditions such as cognitive impairment (sometimes referred to as “brain fog”) and fatigue.
The researchers also found that in comparison to people who did not have COVID, those who did were more likely to experience conditions affecting their nervous system, respiratory function, and circulation, and more likely to feel fatigued or have joint pain.
“It’s not clear what’s behind these symptom variations,” said Dhruv Khullar, M.D., a study author and physician and assistant professor of health policy and economics at Weill Cornell Medicine, New York City. “We hope this work draws attention to possible differences across racial and ethnic groups, stimulates research into the potential mechanisms, and sparks discussion among patients, clinicians, and policymakers.”
In the second study, which published in BMC Medicine, researchers analyzed data from the electronic health records of 33,782 adults and children who received a diagnosis for long COVID between October 2021 and May 2022 at one of 34 U.S. medical centers. All had been given a diagnosis—Post COVID-19 condition, unspecified—the code for the condition first introduced in U.S. health care systems in October 2021.
In studying the profile of these patients and their symptoms, the researchers found multiple patterns. Among the more striking: most of the patients were white, female, non-Hispanic, and likely to live in areas with low poverty and greater access to health care.
Given what researchers already knew about the disproportionate impact of COVID on people of color and economically disadvantaged populations, the findings stood out. Emily Pfaff, Ph.D., a study author and assistant professor in the Division of Endocrinology and Metabolism at the University of North Carolina, Chapel Hill, said the pattern suggested that not all patients who have long COVID are being diagnosed.
The reasons vary. In addition to long-documented health disparities based on race and other factors, she said, women are more likely than men to seek health care in general, and patients with the time and resources to access health care tend to be disproportionally represented in clinical data.
“You can see all the different ways these diagnostic codes can provide insight, but they can also skew the whole story,” Pfaff said.
Still, she added, the insights help. She and her team found, for example, that most of the patients with long COVID had just mild to moderate, not severe, symptoms of acute infection. They also discovered that long-term symptoms could be grouped into common clusters—cardiopulmonary, neurological, gastrointestinal, and coexisting conditions—as well as by age.
Children and teens were more likely to experience gastrointestinal and upper respiratory problems, including stomach aches and coughing. Adults ages 21-45 commonly experienced neurological problems, such as brain fog and fatigue. Adults ages 66 and older were more likely to have coexisting conditions, such as heart problems and diabetes, which the authors suspect is more likely present because of age than long COVID.
The authors of both papers said additional studies are needed to confirm and further categorize these trends.
“This research contributes to our understanding of symptom clusters in long COVID that may be differentiated by race, ethnicity, and influenced by social determinants of health,” said Gary H. Gibbons, M.D., director of the National Heart, Lung, and Blood Institute. “It also provides vital insights into the utility, as well as the constraints, of the diagnostic code now in use for long COVID.”
More information:
Dhruv Khullar et al, Racial/Ethnic Disparities in Post-acute Sequelae of SARS-CoV-2 Infection in New York: an EHR-Based Cohort Study from the RECOVER Program, Journal of General Internal Medicine (2023). DOI: 10.1007/s11606-022-07997-1.
Emily R. Pfaff et al, Coding long COVID: characterizing a new disease through an ICD-10 lens, BMC Medicine (2023). DOI: 10.1186/s12916-023-02737-6
Journal information:
Journal of General Internal Medicine
,
BMC Medicine
Source: Read Full Article